A Joint by Joint Approach to Training
Michael Boyle
"We get old too soon and smart too late." Swedish Proverb
My good friend, Physical Therapist Gray Cook, has a gift for simplifying complex topics. I envy his ability to succinctly take a complicated thought process and make the idea appear simple. In a recent conversation about the effect of training on the body, Cook produced one of the most lucid thought processes I have ever heard.
Gray and I were discussing the findings of the Functional Movement Screen (www.functionalmovement.com), the needs of the different joints of the body, and how the function of the joints relates to training. One of the beauties of the Functional Movement Screen is that the screen allows us to distinguish between issues of stability and those of mobility. Cook's thoughts were simple and led me to realize that the future of training may be a joint-by-joint approach rather than a movement-based approach.

Gray's analysis of the body was a straightforward one; in his mind, the body is a just a stack of joints. Each joint or series of joints has a specific function and is prone to specific, predictable levels of dysfunction. As a result, each joint has specific training needs. The table below looks at the body on a joint-by-joint basis from the bottom up:

A full squat with full mobility
Joint Primary Training Needs:
- Ankle mobility (particularly sagittal)
- Knee stability
- Hip mobility (multi-planar)
- Lumbar Spine stability
- T-Spine mobility
- Gleno-humeral stability
The first thing you should notice as you read the above table is that the joints simply alternate mobility and stability. The ankle needs increased mobility, and the knee needs increased stability.
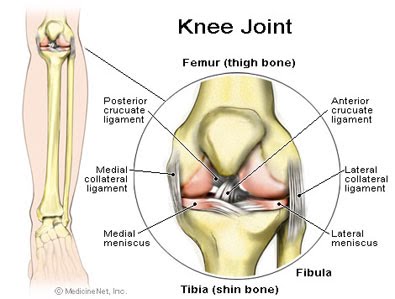
The knee needs stability
As we move up the body, it becomes apparent that the hip needs mobility. And so the process goes up the chain: a simple, alternating series of joints. Over the past twenty years, we have progressed from the moronic approach of training by body part (sorry, bodybuilders) to a more intelligent approach of training by movement pattern. In fact, the phrase "movements not muscles" has almost become an overused one and, frankly, that is progress.
I think most good coaches and trainers have given up on the old chest-shoulder-triceps thought process and moved forward to a push-pull-hip extend- knee extend thought process. Interestingly enough, I now believe the "movement not muscles" process probably should have gone a step further. I think that injuries relate closely to proper joint function or more appropriately to joint dysfunction. Confused? Let me try to explain. Problems at one joint usually show up as pain in the joint above or below.

The hips need mobility
The hips need mobility The simplest illustration is in the lower back. It seems obvious based on the advances of thee part decade that we need core stability and also obvious that lots of people suffer from back pain. The interesting part lies in the theory behind low back pain. My theory of the cause? Loss of hip mobility. Loss of function in the joint below (in the case of the lumbar spine, the hip) seems to affect the joint or joints above (lumbar spine). In other words, if the hip can't move, the lumbar spine will. The problem is that the hip is built for mobility, and the lumbar spine for stability. When the supposedly mobile joint becomes immobile, the stable joint is forced to move as compensation, becoming less stable and subsequently painful.
The process is simple:
- -Lose ankle mobility, get knee pain.
- -Lose hip mobility, get low back pain.
- -Lose thoracic mobility, get neck and shoulder pain (or low back pain).
Looking at the body on a joint-by-joint basis beginning with the ankle, this thought process seems to make sense. An immobile ankle causes the stress of landing to be transferred to the joint above: the knee. In fact, I think there is a direct correlation between the stiffness of the basketball shoe and the amount of taping and bracing that correlates with the high incidence of patellafemoral syndromes in basketball players. Our desire to protect the unstable ankle comes with a high cost. We have found that many of our athletes with knee pain have corresponding ankle mobility issues. Many times this follows an ankle sprain and subsequent bracing and taping.
The exception to the rule seems to be at the hip. The hip can be both immobile and unstable, resulting in knee pain from the instability (a weak hip will allow internal rotation and adduction of the femur) or back pain from the immobility. How a joint can be both immobile and unstable is the interesting question.
It seems that weakness of the hip in either flexion or extension causes compensatory action at the lumbar spine, while the weakness in abduction (or, more accurately, prevention of adduction) causes stress at the knee. Poor psoas and iliacus strength and/or activation will cause patterns of lumbar flexion as a substitute for hip flexion. Poor strength and/or activation of the glutes will cause a compensatory extension pattern of the lumbar spine that attempts to replace the motion of hip extension.
Interestingly enough, this fuels a vicious cycle. As the spine moves to compensate for the lack of strength and mobility of the hip, the hip loses mobility. It appears that lack of strength at the hip leads to immobility, and immobility in turn leads to compensatory motion at the spine. The end result is a kind of conundrum: a joint that needs both strength and mobility in multiple planes.
The lumbar spine is even more interesting.

The lumbar spine needs stability
This is clearly a series of joints in need of stability, as evidenced by all the work in the area of core stability. Strangely enough, the biggest mistake I believe we have made in training over the last ten years is engaging in an active attempt to increase the static and active ROM of an area that obviously craves stability. I believe that most if not all of the many rotary exercises done for the lumbar spine were misdirected. Both Sahrmann (Diagnosis and Treatment of Movement Impairment Syndromes) and Porterfield and DeRosa (Mechanical Low Back Pain: Perspectives in Functional Anatomy) indicate that attempting to increase lumbar spine ROM is not recommended and potentially dangerous. (Is Rotation Even A Good Idea?) I believe our lack of understanding of thoracic mobility has caused us to try to gain lumbar rotary ROM; this is a huge mistake.
The thoracic spine is the area about which we seem to know least. Many physical therapists seem to recommend increasing thoracic mobility, though few seem to have exercises designed specifically for thoracic mobility. The approach seems to be "we know you need it, but we're not sure how to get it." I think over the next few years we will see an increase in exercises designed to increase thoracic mobility. Interestingly enough in Diagnosis and Treatment of Movement Impairment Syndromes, physical therapist Shirley Sahrmann advocated the development of thoracic mobility and the limitation of lumbar mobility.
The gleno-humeral joint is similar to the hip. The gleno-humeral joint is designed for mobility and therefore needs to be trained for stability. I think the need for stability in the gleno-humeral joint presents a great case for exercises like Stability Ball and BOSU Push-ups as well as unilateral dumbbell work.
The inability of joints to function normally places stress on the joints above or below. In the book Ultra Prevention (actually a nutrition book), the authors describe our current method of reaction to injury perfectly. Their analogy is simple; our response to injury is like hearing the smoke detector go off and running to pull out the battery. The pain, like the sound, is a warning of some other problem. Icing a sore knee without examining the ankle or hip is like pulling the battery out of the smoke detector.
What we need to realize is that, as the opening quote says, "we get old too soon and smart too late". Every day, I learn more and more about the body. What I learn allows me to be a better coach and a better educator. Often, what I learn contradicts what I formerly believed. Just remember, the world was once thought to be flat.
Nenhum comentário:
Postar um comentário